
Heart Attack Without Blocked Arteries
-
- Dr. Junaid Arshad
- December 7, 2021
- 1 comments
Table of Contents
INTRODUCTION
Heart Attack without blocked arteries is called MINOCA in medical terminology.
MINOCA stands for Myocardial Infarct with Non-Obstructive Coronary Arteries.
DEFINITION
It is defined as the evidence of a Heart Attack (Myocardial Infacrt or MI) with normal or near-normal blood vessels on an angiogram. (narrowing of ≤50%)
The evidence of heart attack includes chest pain along with any of the following:
- Positive cardiac biomarkers like troponin T/I detetced on blood test
- EKG or ECG changes suggestive of MI
- Imaging evidence like decresed contractility of a segement of heart on echocardiography
Diagnoses of MINOCA cannot be made without an angiogram.
How many people suffer a heart attack without blocked arteries?
Around 6% of people who suffer a Heart Attack are found to have no blockage in the coronary arteries on angiogram and are classified as MINOCA or MI with unobstructive coronary arteries.
However, there are wide variations in these statistics among different studies.
Which is more dangerous. Heart attack with blockage or wihout blockage?
Heart attack without blocked arteries is less dangerous and has a better survival rate.
Studies have shown that in-hospital mortality (death rate during hospital stay) in patients without blockage was 1.1% as compared to 3.2% in patients with blocked arteries.
Similarly, mortality after one year was 3.5% in patients without blockage as compared to 6.7% in patients with blocked arteries.
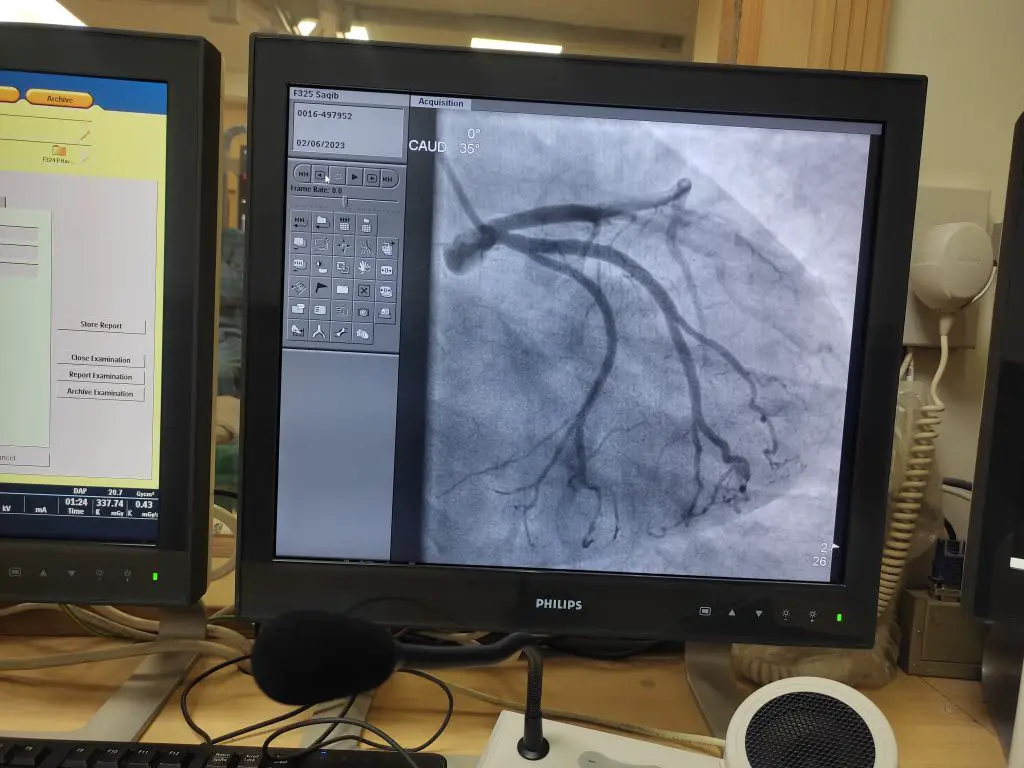
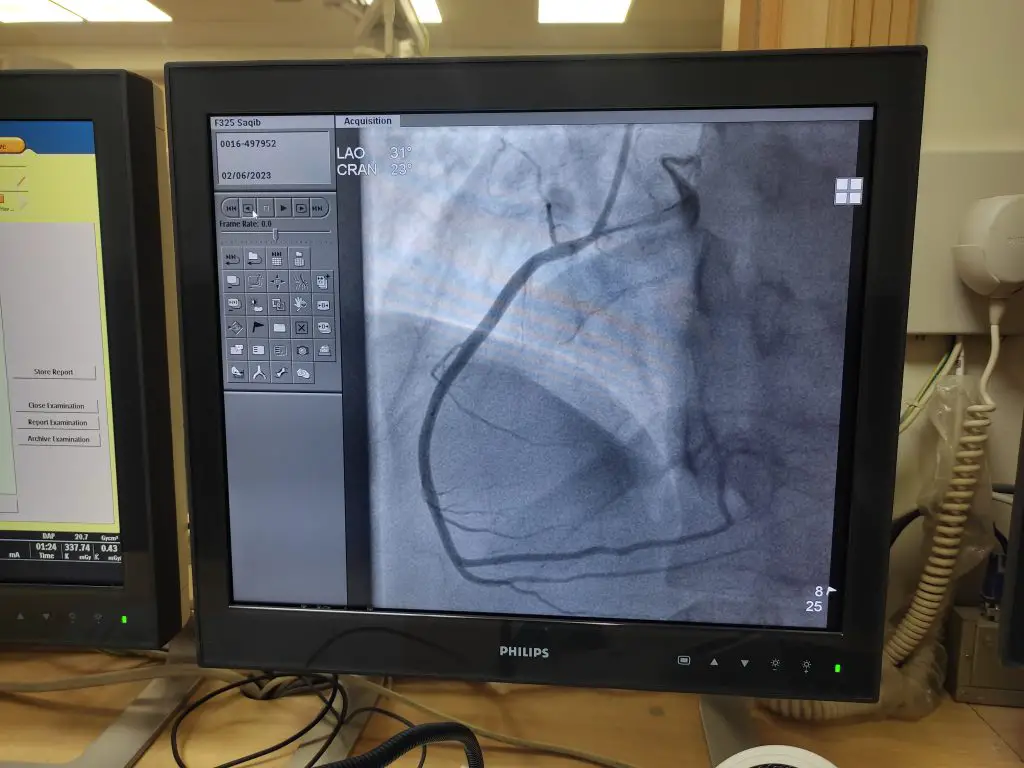
Angiographic images of Normal Coronary Arteries
5 Causes of Heart Attack Without Blocked Arteries
#1. Coronary Artery Spasm
Coronary artery spasm is one of the causes of a heart attack without blocked arteries.
The blood vessels of the heart have no narrowing due to atherosclerosis but they undergo spasm that cuts off the blood supply to a region of the heart & causes chest pain.
The number of patients having MINOCA due to arterial spasm is highly variable & can range from 3%-95%.
Geographical differences can be one of the reasons for this high level of variation in the prevalence of coronary artery spasm as the Asian population is more affected as compared to Caucasians
#2. Spontaneous coronary artery dissection (SCAD)
SCAD is another possible cause of MINOCA.
It is characterized by a separation in the walls of the coronary artery.
For image click here.
Although it causes obstruction in the coronary vessels but there is no atherosclerosis.
It occurs more commonly in young people, predominantly in women.
Statistics say that 87%-95% of patients with SCAD are women.
According to a study, it is a cause of heart attacks in 4% of the general population & 35% of women who are less than 50 years of age.
Causes of SCAD include the following
- Genetics
- Hormonal fluctuations
- Pregnancy
- Extreme stress (physical or emotonal)
#3. Takotsubo or stress cardiomyopathy
It is also called broken heart syndrome or apical ballooning syndrome.
It is characterized by decreased function or contractility of a specific region of the heart & is transient in nature.
Stress cardiomyopathy specifically affects the left ventricle of the heart and it mimics a heart attack.
The precipitating factor is quite often but not always emotional or physical stress.
Emotional stress factors may include the death of a close relative, a huge financial loss, or some natural disaster.
EKG changes and blood tests like troponin T/I show similar results as an obstructive MI.
Unlike obstructive MI, takotsubo or stress cardiomyopathy involves multiple regions of the heart simultaneously & this is one of the clues that help in diagnosis.
Angiography shows normal unobstructive coronary vessels.
The abnormalities produced are transient and patients undergo complete recovery.
#4. Small vessel disease (Microvascular dynsfunction)
A heart attack usually occurs due to the involvement of large blood vessels of the heart.
Angiography can visualize only those large vessels.
Very small vessels called micro-vessels cannot be seen on angiography.
The involvement of micro-vessels can also cause anginal pain & is given the name of Syndrome X.
Angiography shows normal unobstructive coronary vessels.
#5. Viral Myocarditis
Viral Myocarditis is responsible for 1/3rd of the cases of MINOCA & is most commonly caused by adenoviruses, parvovirus B19 (PVB19), human herpesvirus 6, and Coxsackie virus.
Clinical Presentation
The clinical presentation of patients without blocked arteries is similar to those with blocked arteries.
Age and gender make a little difference.
As mentioned previously, patients with MINOCA are young with women being affected more than men.
The conventional risk factors like diabetes, hypertension, smoking, & family history are similar in both groups.
The only exception is raised lipid level or hyperlipidemia which is less prevalent in the MINOCA group. (21% as compared to 32% in patients with obstructive disease.)
Cardiac biomarkers like troponins, EKG, & echocardiography show similar abnormalities in patients with blocked arteries and those without blocked arteries.
How MINOCA is Diagnosed?
Diagnosis of MINOCA involves two things.
Establishing the the diagnosis of MINOCA
Angiography
First of all diagnosis of heart attack is made by ekg, blood tests like trop I/T, & echocardiography.
Once the diagnosis of heart attack is made, the diagnosis of MINOCA is made on angiography that shows normal or almost normal coronary vessels having narrowing of 50% or less.
Diagnosing the underlying cause of MINOCA
CMR
CMR is the key investigation for diagnosing the cause of MINOCA.
It is the MRI of heart that can diagnose structural abnormalities as well as ischemia.
According to European Society of Cardiology ESC 2020 NSTEMI guidelines, CMR can diagnose 87% of the causes of MINOCA including myocarditis & takotsubo cardiomyopthy.
Intracoronary Acetylcholine
This is a test to diagnose the spasm in coronary vessels.
Acetylcholine is gven directly into the coronary vessels.
Ergonovine is an alternate agen that can also be used.
Both of these tests have been recommended by the ESC for the workup of MINOCA.
IVUS/OCT
Both and IVUS & OCT are advanced imaging modalities used in cardiology.
In case of MINOCA they can be used for diagnosing SCAD.
IVUS refers to intravscular ultrasound, also called endovascular ultrasound or intravascular echocardiography.
OCT or Optical Coherence Tomography can take high definition images of coronary arteries & contributes its diagnostic role.
Despite of all these diagnostic advancements, the cause of MINCOA remains undiagnosed in 8-25% of cases.
Treatment of MINOCA
MINOCA is treated with drug therapy.
Unlike Obstrcutive coronary artery disease, no intervention like stenting or CABG is done.
Medication are as below.
- Dual Anti Platelet drugs i.e., Aspirin & clopidogrel
- ACE Inhbitors/ ARBs
- Beta-Blockers like bisoprolol or metoprolol
- Statins (lipid lowering drugs)
Treatment with above mentioned drugs has shown to reduce mortality, acute MI, & stroke.
Summary
Heart Attack with unblocked arteries is a known entity that effects 6% of patients suffering from MI and is called MINOCA (myocardial infarct with non-obstructive cornoaries). It is less dangerous with low mortality rate as compared to obstructive cornary artery disease & effects women more than men. Diagnosis is confirmed with a normal angiogram and CMR can detect the underlying cause in 87% of the cases. Medical therapy is the mainstay of treatment & it reduces mortality.
Hi, I'm Dr. Junaid Arshad
Latest Posts
-

-

Can You Use Expired Glucometer Test Strips? What You Need to Know
December 7, 2021 -

-


1 comment